The New PENTACAM AXL Wave for Refractive Cataract Surgery
BY THOMAS KOHNEN, MD, PHD, FEBO, — Given the high expectations of today’s cataract surgery patients to achieve excellent vision at all distances, we are now tasked with providing refractive precision as the standard of care.
But achieving great results with refractive cataract surgery requires much more than simple biometry and collecting the basic measurements of axial length and anterior surface keratometry. We now need a device that can also measure the posterior corneal surface, anterior chamber depth, and optical biometry.
In my experience, one of the best technologies for all these functions is the Pentacam AXL (OCULUS).
The latest model, the Pentacam AXL Wave, includes a Hartmann-Shack wavefront sensor to measure total eye aberrations and objective refraction, as well as retroillumination for preoperative assessment of crystalline lens opacities in the nondilated pupil and postoperative control of IOL position and inclination.
In all, this one device performs five major functions in one measurement routine on the same measuring axis and using the same alignment navigation: objective refraction, total eye wavefront, retroillumination, optical biometry, and anterior segment tomography.
This is especially practical and helpful in this time of COVID-19 restrictions, as it means there are fewer devices for us to use and sterilize in between patients.
CLINICAL BENEFITS IN PRE- AND POSTOPERATIVE ASSESSMENTS
The Pentacam AXL Wave has not only the practical benefits outlined above, but it also has clinical benefits that I have found especially valuable in preoperative assessments for refractive cataract surgery.
I can perform an objective refraction on every patient, identify any higher-order aberrations (HOAs), and obtain one wavefront to achieve aberration measurements for all eye segments including the total cornea, total eye, and crystalline lens or IOL.
It uses two different pupil diameters (mesopic and scotopic), which is required when implanting a multifocal IOL or performing laser refractive surgery. Further, the anterior segment tomography function can be used to screen for glaucoma, ectasia, and Fuchs endothelial dystrophy, to name a few.
I can also use the Pentacam AXL Wave to assess the visual disturbance and identify its cause (ie, the cornea or the lens). Lastly, it can be used to perform optical biometry and IOL power calculation.
There are also clinical benefits in the postoperative period. I can repeat the objective refraction, recheck for HOAs including spherical aberration and coma, use retroillumination of the pseudophakic eye to depict the multifocal or toric IOL, perform wavefront aberrometry, and assess the postoperative visual performance.
RELIABILITY
We’ve also found the Pentacam AXL Wave to be reliable. In a retrospective, consecutive case series of refractive cataract surgery performed in 20 phakic and pseudophakic eyes, we concluded that the device provided high repeatability of the total root mean square and third- and fourth-order HOAs (0.04 µm for a pupil diameter ≤ 4 mm; 0.05 µm for a pupil diameter of 5 mm). We also looked at the comparability of subjective and objective refraction in 21 pseudophakic and phakic eyes.
In this retrospective, consecutive case series, we took three consecutive measurements with the Pentacam AXL Wave and the iTrace (Tracey Technologies). We found high correlation with the objective measurements of both devices to the subjective refraction performed by a trained optician (Pentacam AXL Wave, 1.58 vs 1.61 D; iTrace, 1.96 vs 1.56 D).
We concluded that the correlation was better with the Pentacam AXL Wave and that both devices offer a good coefficient of variation (Pentacam AXL Wave, 0.11 vs iTrace, 0.14). This translates to reliable measurements and high repeatability.
CONCLUSION
Providing patients with refractive accuracy after cataract surgery is no longer a bonus to patients, it is expected every time.
The most important consideration in ensuring that we can achieve these results is to incorporate precise, repeatable, reliable measurements in the pre- and postoperative periods. In my experience and clinical studies, I have been impressed with the Pentacam AXL Wave to provide this level of precision.
Having access to one device that performs five very important functions in one measurement routine is practical and economical. The Pentacam AXL Wave has become an indispensable tool for better and faster measurements in refractive cataract surgery.
Pentacam AXL Wave: A Cost-Benefit Analysis — An all-in-one system that in our minds is worth every penny.
BY GERD U. AUFFARTH, MD, PHD, FEBO; AND MAXIMILIAN HAMMER, BSC, — We all have the same overarching goal as physicians, and that is to take optimal care of our patients using the most appropriate therapies and surgical methods.
This, however, entails making a significant investment in technologies and answering the fundamental question of cost and benefit in all investments. Does the investment truly increase effectiveness, or is it just nice to have?
Does the marketing promise stand up to the clinic routine? Can one system really do it all? Can the investment be adapted to current and also future needs? This article presents our view on the Pentacam AXL Wave (OCULUS), one of four available models of the Pentacam family.
ONE DEVICE, A MULTITUDE OF APPLICATIONS
The first question in the cost-benefit analysis should be its clinical benefits. The Pentacam AXL Wave can be used for corneal surgery, refractive lens surgery, presbyopia correction, and standard cataract surgery.
Corneal, cataract, and presbyopia surgery.
The Pentacam is not the only diagnostic device that measures the anterior and posterior corneal surface and the total corneal thickness, but it currently provides the best repeatability.
It also incorporates the Belin/Ambrósio Enhanced Ectasia Display, which is helpful to detect early ectatic diseases, which is essential for corneal refractive surgery.
The Belin ABCD keratoconus staging and progression system, which independently evaluates the anterior and posterior corneal surfaces, the thinnest part of the cornea, and the distance corrected visual acuity.
This is an indispensable tool when CXL treatments are indicated. Corneal dystrophies and several other abnomalities can be detected with the Fast Screening Report, which is based on scientific data.
Combining this information with the detection of forme fruste keratoconus using the Belin/Ambrósio software provides a solid decision basis for presbyopia correction with multifocal IOLs.
The Cataract Pre-OP Display provides a straightforward IOL selection process. With the Pentacam AXL Wave, Scheimpflug tomography, optical biometry, total eye wavefront, objective refraction, and retroillumination imaging are captured in one process that takes less than 5 minutes for both eyes.
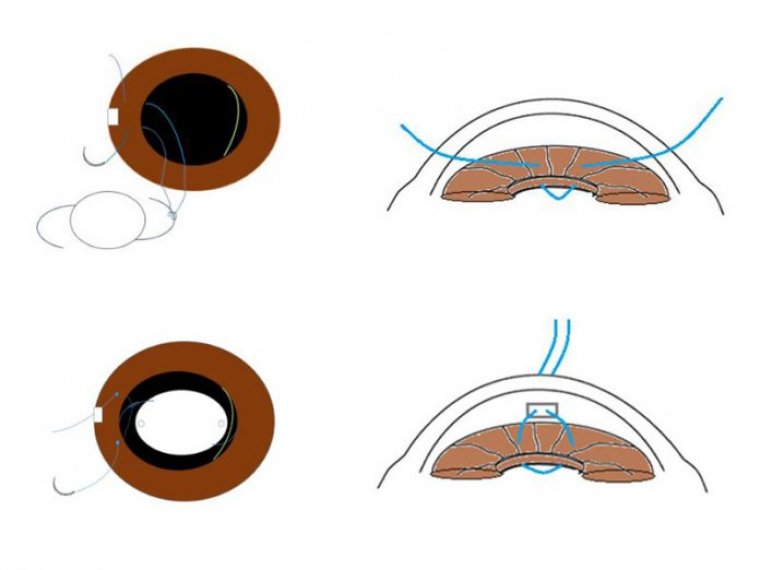
This shortens our examination time and increases workflow. Refractive lens surgery. The Pentacam AXL Wave offers software-based planning for iris-fixated phakic IOLs. Moreover, all parameters needed for phakic lens selection and calculation are shown in the Overview Display and the Cataract Pre-OP Display.
According to the literature, the Pentacam provides the most accurate measurement of corneal diameter in terms of repeatability and comparability for phakic IOL sizing.
MORE QUESTIONS ANSWERED
The Pentacam AXL Wave serves many purposes, but there are still questions to be answered during the cost-benefit analysis.
Which IOL calculation formulas offer the best results? Can the device help to determine patient candidacy for a specific IOL? Is a standalone optical biometer really enough? IOL calculations.
Most modern IOL power calculation formulas either estimate the influence of the posterior corneal surface (eg, Barrett toric with estimated PCA) or use the measured corneal posterior surface (eg, Barrett Toric with measured PCA).
The Savini calculator uses the total refractive power of the cornea to calculate the toricity. Besides these formulas, the Pentacam AXL Wave a
lso contains the Hoffer Q, Holladay 1, SRK/T, Haigis, double-K, Barrett True-K, Barrett Universal 2, and the Olsen ray-tracing formulas in the Pentacam IOL Calculator.
Another special feature is the IOL database, which includes the IOL constants, delivery areas, and optical designs for about 500 different IOLs. This avoids time consuming collection of IOL data. Patient candidacy.
When selecting the best IOL (eg, aspheric or multifocal), mesopic and scotopic pupil diameter cannot be neglected. The Pentacam AXL Wave takes measurements at both pupil sizes, ensuring the most accurate results. One device is enough.
The total eye wavefront, objective refraction, and retroillumination are displayed (Figure) at the top of the Pentacam AXL Wave’s Overview Display. We recently compared the Pentacam AXL Wave with the ARK 1s (Nidek) and the ORK-CAM (Schwind eye-tech-solutions).
We found an almost identical repeatability and comparability of the Pentacam AXL Wave and the ARK 1s in phakic, pseudophakic, and keratoconic eyes, and we concluded that the ARK 1s and the Pentacam AXL Wave are interchangeable.
However, the Pentacam AXL Wave has an additional advantage because it can be used to take refractive measurements, which helps to save valuable clinic time. We also found that the Pentacam AXL Wave had better repeatability than the ORK-CAM to determine spherical aberrations, and the mean value was almost identical.
Therefore, the ORK-CAM and AXL Wave are interchangeable. CONCLUSION The Pentacam AXL Wave gathers all the information you need for preoperative diagnostics, patient education, and surgical planning and postoperative assessment in one measurement procedure for the entire spectrum of corneal and cataract surgery.
For the reasons outlined here, we do believe that the Pentacam AXL Wave is worth the investment.
IOL Power Calculation With the Pentacam AXL Wave — A powerful, time-saving solution for preoperative workups.
BY GIACOMO SAVINI, MD, — Patients today expect nothing less than high-quality vision after cataract surgery.
Therefore, the requirements of our care are continually increasing, and it is imperative that we have accurate and reliable ocular diagnostics technologies that can help us to select the appropriate IOL power.
The Pentacam AXL Wave (OCULUS) can be used like any other optical biometer to calculate the IOL power, with the advantages of using state-of-the-art Scheimpflug technology and Hartmann-Shack aberrometry.
With the Pentacam AXL Wave, the average keratometry, anterior chamber depth, lens thickness, and axial length can be entered into the Barrett Universal II, Haigis, Hoffer Q, Holladay, and SRK/T formulas to determine IOL power.
Alternatively, the Olsen ray-tracing formula, which uses information from the posterior cornea, can also be used with the Pentacam AXL Wave. THREE ADVANTAGES The Pentacam AXL Wave has three distinct advantages.
No. 1: Excellence in refractive results. With the Barrett Universal II formula, 86.8% of eyes achieved a prediction error within ±0.50 D and a median absolute error of 0.240 D. All eyes were implanted with an AcrySof SN60WF (Alcon).
In larger studies with the same IOL, the percentage of eyes achieving the same prediction error ranged from 72.3% to 82.9%.2-4 In these studies, the IOLMaster 500 (Carl Zeiss Meditec) or the Lenstar LS 900 (Haag-Streit) were used.
Interestingly, unpublished data showed that the results with the Pentacam AXL Wave were even better in a preliminary study of 63 eyes implanted with the PanOptix IOL (Alcon). The percentage of eyes with a prediction error of ±0.50 D was as high as 92.06% (Table).
No. 2: A state-of-the-art Scheimpflug camera. The Scheimpflug camera measures the posterior corneal curvature precisely5 and calculates the total corneal power and astigmatism, which has been shown to be more accurate than standard keratometric astigmatism.
The resulting toricity of the IOL is calculated by the Savini Toric Calculator, available in the IOL calculation display. In post-LASIK eyes, we recently demonstrated that using the posterior corneal curvature data from the Pentacam AXL significantly improves the refractive outcomes of the Barrett True-K formula, which is included in the IOL calculator of the Pentacam AXL Wave.
In a sample of 50 eyes of 50 patients, as many as 70% achieved a prediction error within ±0.50 D.7
The Cataract Pre-OP Display provides essential information for IOL selection, including:
• The total corneal higher-order aberrations (when these are >0.3 µm, diffractive multifocal IOLs should not be chosen);
• Corneal maps including posterior corneal curvature measurements to show regularity of astigmatism for toric IOLs;
• The total corneal spherical aberration at 6 mm, which is useful when selecting aspheric IOLs with different degrees of negative spherical aberration; and
• The comparison of keratometric and total corneal astigmatism, which is useful with toric IOLs.
No. 3: The introduction of Hartmann-Shack aberrometry. Hartmann-Shack aberrometry is particularly useful when it is difficult to understand whether the visual disturbances come from the cornea or the lens.
Other aberrometers can do a similar task, but they are based on Placido-disc technology, which do not include posterior corneal measurements into the internal visual quality.
CONCLUSION Having tested almost every biometer and tomographer available today, I have to conclude:
The Pentacam AXL Wave with its combination of Scheimpflug tomography, optical biometry, Hartman-Shack aberrometry and retroillumination supports me the best in selecting the right IOL power, which in turn helps me to achieve excellent refractive results for my patients.