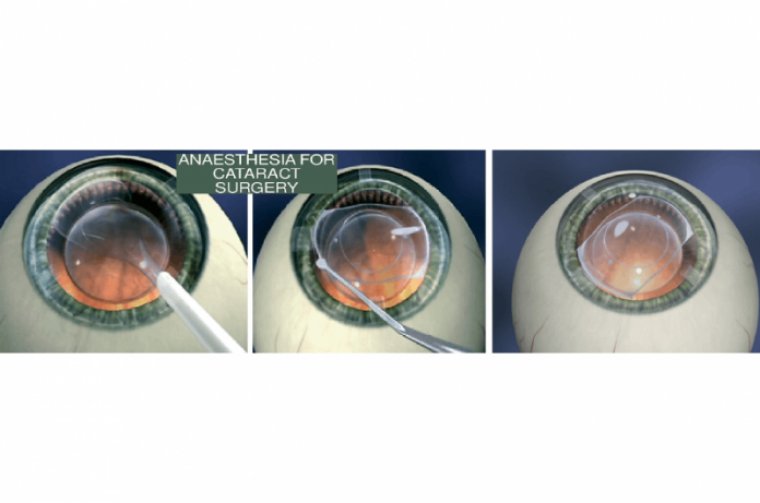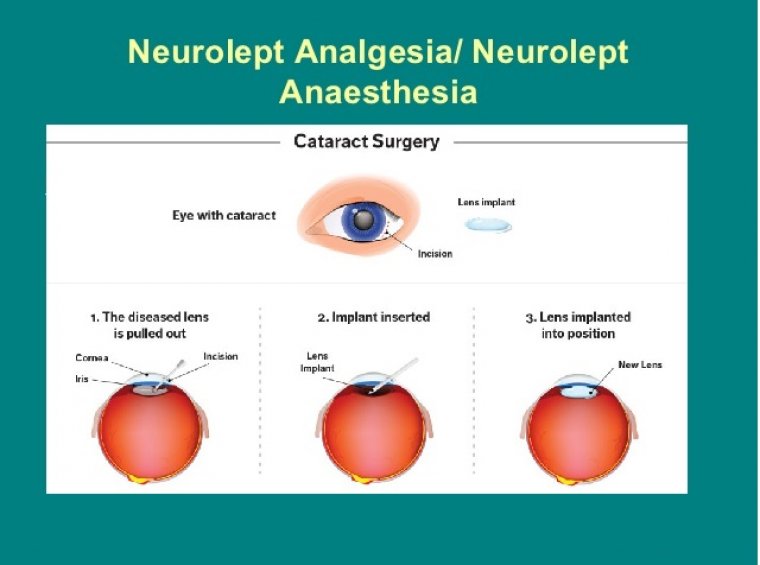
Cataract Surgery & Neurolept Anesthesia
Neurolept anesthesia is a technique of general anesthesia based on intravenous administration of neuroleptic drugs, together with inhalation of a weak anesthetic with or without neuromuscular relaxants.
Neurolept anesthesia produced by droperidol, fentanyl, N2O-O2, and a muscle relaxant is a commonly used anesthetic technique, especially in the more severely medically compromised patient
The timing of administration of neurolept anesthesia for refractive laser-assisted cataract surgery does not seem to affect patients’ perception of pain.
Findings from a recent study showed no difference in the pain scores between early and standard administration of anesthesia on postoperative day 0 (POD0) and postoperative week 1 (POW1), reported Rishi Gupta, BSc, lead study author from the University of Ottawa Faculty of Medicine in Canada.
Refractive laser-assisted cataract surgery is a 2-phase event, ie, application of a femtosecond laser followed by the manual portion of the surgery.
The authors theorized that the timing of the anesthesia administration may affect the patients’ perception of pain, explained Sohel Somani, MD, FRCSC, senior study author from the Department of Ophthalmology and Vision Sciences at the University of Toronto in Canada.
STUDY DESIGN/FINDINGS
This study was a prospective, randomized controlled trial that included 38 patients who received anesthesia at the standard time (defined as after completion of the refractive laser-assisted cataract surgery and immediately before the draping of the eye) and 35 patients who received early administration of anesthesia (defined as before the start of the laser-assisted cataract surgery).
The primary outcome was the pain scores using the visual analog scale on POD0 and POW1. The secondary outcomes were the baseline ocular data, surgical parameters, anesthesia doses, vital signs, and anxiety scores.
The investigators found that the preoperative heart rate, intraoperative mean arterial pressure, and postoperative heart rates differed significantly between the 2 cohorts, with significantly higher rates seen at all time points (P = .02, P = .04, and P = .04, respectively) in the early administration group.
Interestingly, no differences in pain scores between the 2 patient cohorts were seen at the 2 postoperative time points. However, and even more interestingly, the anterior chamber depth was a highly significant factor in this study.
The data showed that when considering all patients, each 1-mm increase in the anterior chamber depth caused an increase of 1.51 pain units (P = .007) at the evaluation on POW1.
Regarding the pain scores at that same time point in all patients, the second eye had an increase of 0.71 pain unit (P = .02) compared with the first eye.
“Anterior chamber depth was correlated strongly with the pain perceived at the POW1 evaluation, which indicates the need for future research to assess the relationship between pain and the anterior chamber depth,” the authors commented.
They also advised that the dose of midazolam being administered can be increased to alleviate the patients’ pain associated with the increased anterior chamber depth.