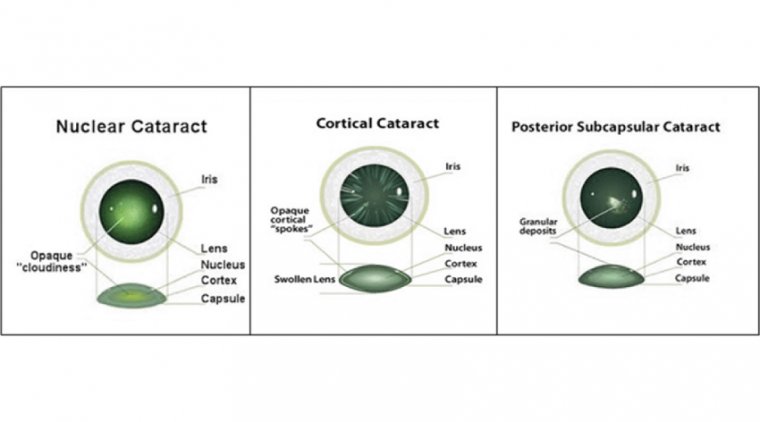
Subcapsular Cataract
Anterior subcapsular cataract lies directly under the lens capsule and is associated with fibrous metaplasia of the lens epithelium.
Posterior subcapsular opacity lies just in front of the posterior capsule and has a granular or plaque-like appearance on oblique slit lamp biomicroscopy, but typically appears black and vacuolated on retroillumination.
The vacuoles are swollen migratory lens epithelial cells (bladder or Wedl), similar to those commonly seen postoperatively in posterior capsular opacification.
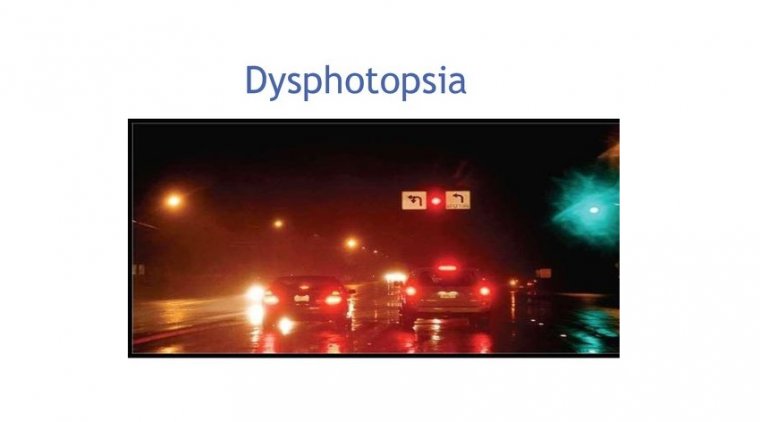
Due to its location at the nodal point of the eye, a posterior subcapsular opacity often has a particularly profound effect on vision.
Patients are characteristically troubled by glare, for instance from the headlights of oncoming cars and symptoms are increased by miosis, such as occurs during near visual activity and in bright sunlight.
Anterior subcapsular cataracts (ASC) form after anterior lens epithelial cells become necrotic from a variety of causes including iritis, keratitis, inflammation associated with atopic dermatitis, irradiation, or electrical burns.
The opacification of the lens is due to a migration of adjacent epithelial cells into the damaged area and subsequent transformation of these cells into a plaque of multiple layers of myofibroblasts.
The most posterior layer of these cells remain epithelial cells and will produce a new lens capsule.
Over time the myofibroblasts resolve leaving a wrinkled appearance to the lens capsule. A duplication cataract occurs when a cortical cataract develops in the same area as the ASC.
Emerging Cataract Surgery Technologies in the ASC
Compact, single-use phaco units that fit in the palm of your hand. Femtosecond lasers integrated with sensor-based, automated cornea-marking capability. Three-dimensional displays that eliminate the back and neck pain associated with performing cataract surgery day after day.
Whether you’re looking to update existing equipment or considering a new purchase to stay on the cutting edge, the latest innovations in cataract surgery offer ASCs and their surgeons more options than ever.
New Kids on the Block: miLOOP and Zepto
Perhaps nowhere is this more evident than with the recent appearance of two micro-interventional devices designed specifically for cataract surgery: miLOOP (ianTECH, recently acquired by Carl Zeiss Meditec) and the Zepto capsulotomy system (Mynosys Cellular Devices).
Cleared by the FDA within the past 2 years, both devices are about the size of a large pen and utilize a thin, tiny filament made of nitinol to achieve treatment goals.
In miLOOP’s case, the surgeon loops the wire around and breaks the nucleus into small pieces for elimination with phaco. With Zepto, the surgeon uses the device to perform a capsulotomy. Both are also single-use devices.
“With regard to micro-interventional and cataract fragmentation, the miLOOP is really a game changer with regard to dense cataracts,” says Steve Dewey, MD, an ophthalmologist at Colorado Springs Eye Clinic and the Pinnacle Surgery Center, also in Colorado Springs.
“I’ve always enjoyed the opportunity to work with a cataract that was basically rock hard,” says Dr. Dewey. “The miLOOP sets a new standard” by creating at least one cleavage, and often two or three, prior to engaging the phaco needle with the nucleus, thus reducing phaco power, he says.
Advocates of miLOOP and Zepto also tout their small size, speed, safety, efficiency, as well as lower costs while achieving results comparable to femtosecond laser-assisted cataract surgery (FLACS) in most circumstances.
“miLOOP and Zepto don’t require a large footprint in the OR,” says William F. Wiley, MD, a cataract surgeon with the Cleveland Eye Clinic in Cleveland, OH. “They can be stacked on the shelf and provided to the OR as needed.”
Farrell C. Tyson, MD, FACS, owner of Tyson Eye in Cape Coral, FL, agrees that the future of both devices looks bright.
“With the miLOOP, you have a device that really simplifies many of the more difficult cases,” says Dr. Tyson, who says the miLOOP is his “go-to” for most conventional cataract cases in daily practice.
“Therefore,” he continues, “you have fewer complications, which means you’re not utilizing the resources in your OR as heavily. You’re not going to have to pay for more nursing time, and you get in and out. With standard cases, it’s going to speed up the case.”
He says the Zepto, which he used as part of the device’s pre-approval studies, enables surgeons to create a capsulorhexis more precisely, more predictably, and more safely than with a femtosecond laser.
“For some surgeons, that’s a real benefit,” says Dr. Tyson, adding that both devices “make good surgeons great and so-so surgeons good.”
Both the miLOOP and Zepto can also enhance the ASC’s bottom line, says Dr. Tyson, noting that the average surgeon takes 22 minutes to complete a cataract case, according to Medicare statistics. “In my facility, I’m averaging 4.5 minutes a case. So, with two ORs, I can perform eight to 10 cases an hour using miLOOP.”
Phaco: Still Advancing
Although it’s been more than half a century since phacoemulsification made its debut, the technology is far from graying.
“Phaco technology has advanced a great deal,” says William B. Trattler, MD, a cataract eye surgeon at the Center for Excellence in Eye Care in Miami, FL.
“Whether it’s Bausch + Lomb, Johnson & Johnson Vision, or Alcon technologies, what we have today is vastly superior to what was available just 10 years ago,” Dr. Trattler continues. “The fluidics are improved, the ability to break up harder nuclei is better, and there’s less postoperative corneal swelling and faster visual recovery.”
“We do have amazing technology right now,” agrees Larry Patterson, MD, who co-owns Eye Centers of Tennessee with his son, Michael Patterson, DO.
“Back in the ’90s in particular, there were tremendous improvements in the quality of phaco. But in the last 10 years, the improvements have been much more incremental,” Dr. Patterson says.
Indeed, the latest offerings from major phaco makers consist primarily of upgrades to current lines.
Take Bausch + Lomb’s Stellaris Elite, for example. Introduced in 2017, the latest iteration of the company’s popular phaco device features many improvements, such as Adaptive Fluidics and Attune energy management.
“It has great fluidics and great chamber control,” Dr. Patterson says. “I live in a rural area, and although I see a great deal of dense cataracts, I hardly ever run into a cataract that I can’t emulsify rather efficiently with this machine.”
Johnson & Johnson Vision, meanwhile, recently updated its Whitestar Signature Pro system with innovative needle motion and advanced fluidics that provide a choice of peristaltic or Venturi pump capabilities.
“Quite honestly, the armamentarium on the Signature Pro is fantastic,” says Dr. Dewey, citing in particular the unit’s Ellips FX handset for cataract removal — the emulsification tip moves forward and backward and side to side at the same time.
“This allows for a very efficient emulsification with much less heat buildup than we saw with traditional longitudinal phacoemulsification,” he says, offering similar praise for the Signature Pro’s dual vacuum system, which enables surgeons to seamlessly switch between peristaltic and Venturi vacuum during surgical cases.
“This unit is incredibly versatile in being able to handle every case — from the densest rocks to the softest of cataracts,” he says. “It performs wonderfully, even in the most adverse situations — from the smallest of pupils to the shallowest of anterior chambers to the deepest of anterior chambers and more.”
Femto laser, Other Technology
At just about a decade old, phaco’s younger brother, the femtosecond laser, continues to gain adherents despite the technology’s much higher initial cost (an estimated $300,000 vs. an estimated $60,000 per phaco unit) and continuing debate over its cost-effectiveness versus that of conventional phaco.
Major recent developments within the FLACS space include the 2018 FDA approval of Lensar’s IntelliAxis-L-Lensar laser system, which improves toric lens placement by replacing manual corneal marking for capsulotomies with sensor-based, automated marking.
“IntelliAxis is a game-changing technology,” says Dr. Trattler, a fan of FLACS. “It’s much better than manual marking. It saves the surgeon a great deal of time because all of the marking is done by the laser at the time of surgery.”
Dr. Trattler is also excited by Alcon’s Ngenuity system, a high-resolution, three-dimensional display system that relieves surgeons from the microscope during surgery. Instead, they use special glasses to view the action on screen in 3D.
“During surgery, I’m not looking through oculars. Instead, I wear 3-D glasses and view the image on a high-resolution 4K monitor,” he says. “While operating, I am keeping my back nice and relaxed, and my neck is in a comfortable position.”
Healthy Competition Drives Value
With new technologies and updates like these appearing in the marketplace, ASC operators and surgeons alike may feel a degree of pressure to keep up with Joneses. Yet, it’s critical to maintain perspective and balance.
“It’s important that surgeons understand how these techniques or options may fit into their practice, and what is going to provide a better value to them, their ASC, and their patients,” says Dr. Wiley, adding that continuing innovation in cataract surgery technology helps foster healthy competition among manufacturers.
“With multiple options developing, the potential for competition is always good; it tends to drive value by driving better outcomes and, potentially, better value for patients and surgeons,” he says. “It gives surgeons and ASCs the opportunity to investigate alternative methods that might provide better or more precise outcomes at similar or better pricing.”