Cornea - Cataract Surgery & Intraoperative OCT
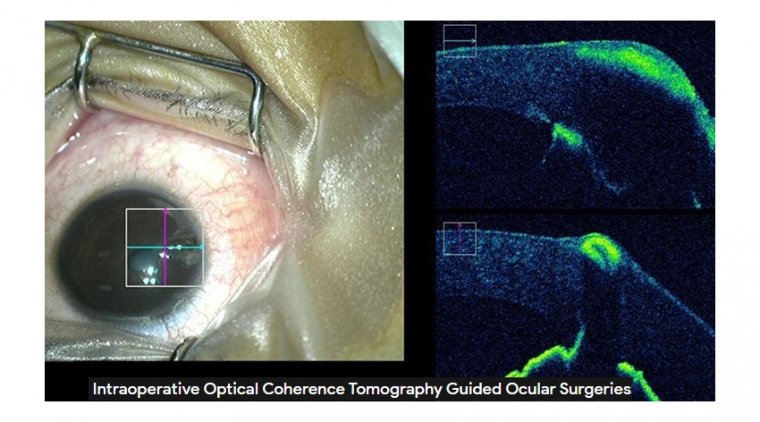
Intraoperative optical coherence tomography (iOCT) is a noninvasive imaging modality that provides a real-time dynamic feedback of the various surgical steps.
The use of iOCT as an aid to decision-making has been successfully reported in cases undergoing keratoplasty, implantable Collamer lens (ICL) implantation as well as cataract surgery. iOCT helps to assess the graft-host relationship in penetrating keratoplasty.
It helps confirm the presence of a big bubble, detect subclinical big bubbles and guide layer by layer stromal dissection in cases of deep anterior lamellar keratoplasty.
It acts as a guide during crucial surgical steps in endothelial keratoplasty, right from scoring of the Descemet membrane to ensuring graft apposition at the end of surgery. The morphological features of the corneal incision in phacoemulsification may be assessed.
iOCT is a useful tool in assessing the status of the posterior capsule and may help identify preexisting posterior capsular defects during cataract surgery in various clinical scenarios such as posterior polar cataract, traumatic cataract, and vitrectomized eyes.
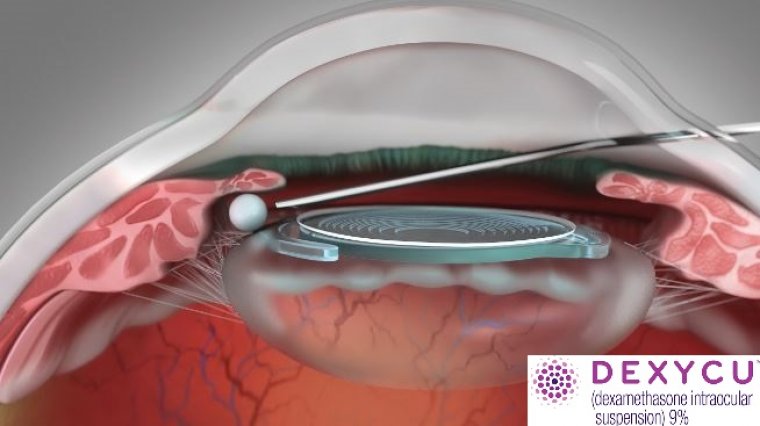
It allows on-table assessment of the ICL vault and potentially facilitates exchange of ICL in the same sitting in extremes of vault.
Ocular surface disorders such as ocular surface squamous neoplasia, pterygium, and dermoid may find an application for iOCT, wherein an iOCT-guided stromal dissection will ensure adequate depth of dissection.
Further technological advancements may allow for automatic centration and tracking and address the present limitation of instrument-induced shadowing.
Having optical coherence tomography (OCT) in the operating room can save time and money, reduce revisions and improve patient outcomes.
“Just like in the office setting, intraoperative OCT can allow you to see structures you can’t normally see with the typical light microscope,” said Dr Francis W. Price Jr., founder of Price Vision Group, Indianapolis, United States and founder/president of the Cornea Research Foundation of America.
“That’s why it shines with endothelial keratoplasty and anterior lamellar surgery.” Manufacturers may have expected intraoperative OCT to find its widest application in retina procedures, but Dr Price said it can be invaluable in the cornea and anterior chamber procedures which fill most of his operating schedule.
Intraoperative OCT can also be helpful in some cataract surgeries, he noted. Lamellar transplants can benefit greatly from the improved imaging provided by intraoperative OCT.
OCT can reduce surgical time for endothelial keratoplasty, particularly Descemet’s stripping endothelial keratoplasty (DSEK) and Descemet’s membrane endothelial keratoplasty (DMEK).
“Intraoperative OCT can be helpful in DSEK by making sure that the graft is in total apposition with the recipient cornea,” Dr Price explained.
“OCT helps you ensure there are no spaces, no abnormalities like Descemet’s membrane that is curled up or stroma that is keeping the graft from adhering.
And you get visual reassurance that your graft is positioned properly and tightly in place.” In DMEK, Intraoperative OCT quickly identifies the orientation of the graft, even in cloudy corneas, Dr Price said.
Fast and positive graft orientation speeds the case as it enhances safety and improves outcomes. “The third type of transplant where intraoperative OCT extremely helpful is deep anterior lamellar keratoplasty,” Dr Price said.
“The gold standard for these procedures is to do a big bubble. But there are cases where you can’t use a big bubble to separate Descemet’s membrane from the rest of the cornea. And sometimes you just can’t get that big bubble to form properly.”
Eyes that have scars from previous cataract surgery are not good candidates for big bubble formation.
Eyes with hydrops, commonly seen with keratoconus, do not do well with big bubbles. Nor do eyes that have had previous radial keratotomy or other procedures that form scars including Descemet’s membrane.
Manual dissection has always been a potential strategy in these eyes, but effective manual dissection is difficult using conventional microscope imaging. The dissection bed must be less than 100 μm deep for excellent visual results following deep anterior lamellar grafts.
Dissection must be uniform, he added. “If you have variable thickness, your visual outcome will be poor,” Dr Price cautioned.
“By using intraoperative OCT, you can have excellent results with your manual dissection without using a big bubble. That’s particularly important in those eyes where you can’t get one.”
Use in Cataract Surgery
Most ophthalmic surgeons work on cataracts, Dr Price noted. Cataract surgeons, too, can work more effectively using intraoperative OCT. OCT does not go through the iris, he said, but it gives a clear view into the anterior chamber.
That gives OCT an advantage in spotting nuclear fragments from very dense cataracts that have lodged in the angle and are less visible through conventional imaging. Dr Price added that OCT is especially useful when the surgeon has used dispersive viscoelastics.
Viscoelastic can be difficult to clear from the angle, even more so when there are dense nuclear fragments present.
Time Saver
Improved imaging can save time in many different transplant procedures, Dr Price said.
He sees the greatest time savings in endothelial keratoplasty. Many surgeons stamp grafts with an “S” to help with final positioning. But the stamp can be difficult to see before the graft is unscrolled, particularly through a cloudy cornea.
Intraoperative OCT clearly images the graft orientation and speeds the procedure. Deep anterior lamellar transplants may not move more quickly using intraoperative OCT, but using it does not slow the surgeon down, Dr Price said.
The improved imaging enhances outcomes and sharply reduces the need to return to the eye with penetrating keratoplasty. Reducing the need for PK revisions gives intraoperative OCT an advantage over conventional imaging.
One advantage of current intraoperative OCT application is the ability to display the image in the ocular. Another useful piece of implementation is the ability to view OCT images as picture in picture with microscope view.
Let's Check What Others Think & Say