Toxic Anterior Segment Syndrome (TASS)
Toxic anterior segment syndrome (TASS) is a severe, acute, sterile intraocular inflammation that occurs the same day or in the early stages after intraocular surgery. It has been most commonly reported after phacoemulsification, keratoplasty, and less frequently, after posterior segment surgeries.
Almost all cases occur after uneventful cataract surgery, and it has been reported after phakic intraocular lens implantation. Previously, this syndrome was defined by many names, such as sterile endophthalmitis or postoperative uveitis of unknown cause.
Furthermore, a condition termed toxic endothelial cell destruction (TECD) syndrome has been described and is now believed to be a variant of TASS.
The overall incidence of TASS was found to be 0.22% in a large case series published by Johnston. Additionally, a significant number of reported cases have occurred as clusters of outbreaks. The origin of this reaction seems to be noninfectious substances introduced into the eye during surgery, producing a breakdown of the blood–aqueous barrier.
Various exogenous chemicals have been identified as the cause of TASS such as residues left behind during cleaning and sterilization of surgical instruments, irrigating solutions with incorrect pH, osmolarity or ionic composition, preservatives, stabilizing agents, denatured ophthalmic viscoelastic devices, endotoxins, heavy metals, intraocular medications at toxic doses, and ointments.
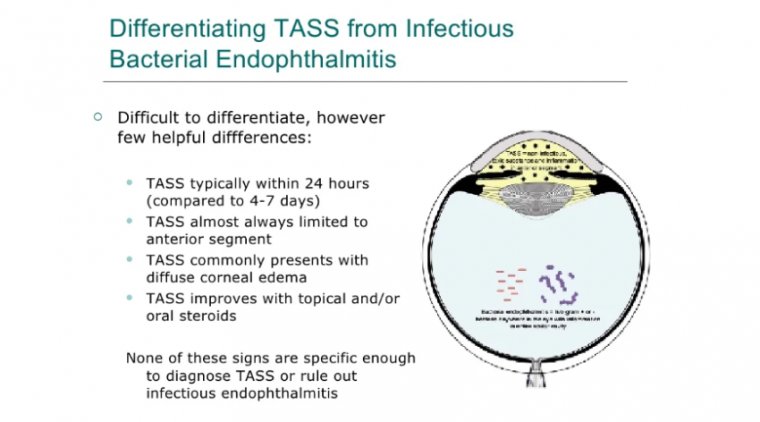
According to the literature, common signs of TASS are presence of cells, flare, and fibrin formation (anterior chamber [AC] inflammatory response); as well as corneal edema without compromising the posterior segment. It is typically characterized by an acute presentation (12–48 h after surgery), without salient complaints of pain.
Given the technological developments in ophthalmic surgery, more intricate and precise surgical instruments are needed, especially micro-instruments, which are slimmer, more delicate, and precise.
These expensive instruments are likely to be damaged or incompletely disinfected during the process of cleaning and packaging. Ophthalmic surgery is difficult to perform and requires a high level of accuracy, such that the performance of surgical instruments has a direct effect on surgical outcomes.
Incomplete sterilization of surgical instruments can have negative effects, such as eye infection. Toxic anterior segment syndrome (TASS), which was first identified by Monson and his coworkers in 1992, is a set of acute anterior chamber aseptic inflammatory reactions that occur within 12 to 24 hours after cataract surgery or other anterior segment surgeries.
In recent years, the incidence of TASS has gradually increased due to increases in phacoemulsification, causing concerns about the handling of instruments for ophthalmic surgery.
Toxic anterior segment syndrome (TASS) is characterized by sterile postoperative inflammation of anterior segment after intraocular surgery. Although TASS most often occurs after cataract surgery, it has also been reported after keratoplasty and posterior segment surgeries.
The inflammation can be mild with a minimal cellular reaction or severe enough to cause marked cornea edema and hypopyon.
During the past 5 years, we have developed an all single-use instrument cataract surgery (ASUICS) custom pack.
The surgical instruments contained in the pack are the only ones used to prepare the surgery tray. We regularly use it for cataracts up to Lens Opacities Classification System III grade 4.
Advantages
Before discussing the contents of this custom pack, let us consider the possible advantages of single-use instruments in cataract surgery. Such discussions are usually based on 3 factors: risk, cost, and the waste materials produced.
Cleaning Instruments
Cleaning any instrument that has a cannular structure, even when the manufacturer’s instructions are thoroughly followed, has the potential to leave microscopic remains lodged inside that could pose a genuine threat to patients or at least worsen outcomes.
In Germany, the Commission on Hospital Hygiene and Infection Protection at the Robert Koch Institute and the Federal Institute for Drugs and Medical Devices suggest mechanical cleaning of reusable instruments or surgical equipment prior to sterilization.
The small inner lumen diameter of phacoemulsification and irrigation/aspiration handpieces does not permit mechanical cleaning with a brush, so compressed air or flushing with water or solvents is required.
However, this is far less thorough than a brush. FDA guidelines recognize that instruments with lumens that are not freely accessible (ie, they have sharp angles or are too small to permit access with a brush) may pose a challenge to adequate reprocessing.
Infection Risks
Using only single-use instruments abolishes the potential risk of infection transmission. Prophylactic intracameral antibiotics may seem a simple solution to the issue, but they have a significant drawback in that they contribute to emerging antimicrobial resistance.
Other drawbacks include, but are not limited to, inefficacy due to dilution, contamination during preparation, toxic anterior segment syndrome, corneal endothelial toxicity, hemorrhagic occlusive retinal vasculitis, and toxic effects on the retina.
Although disposable instruments are generally considered more expensive, reusable instruments have hidden costs including those incurred from reprocessing, maintaining an autoclave facility, cleaning microbicides and instruments for disinfection, packaging, and human resources.
In addition, there are unexpected expenses such as accidental damage/repair, maintenance, and the need to update them to keep pace with technological breakthroughs.
Non-Single-Use
Another factor to consider is that investment in nonsingle-use instruments may have limited the advancement of techniques.
For example, reducing the caliber of an instrument may make it no longer practical to clean and reuse for a sufficient number of times. Thus, reducing the diameter may effectively mean that all instruments are usable only a very limited number of times.
Pack Contents
The custom ASUICS pack includes a nanolaser handpiece, a microscope handle cover, a phacoemulsification cassette, an eyelid retractor, scissors, a side-port blade, a syringe with physiological solution, a syringe, a hydrodissection cannula, a cystotome holder, 2 ophthalmic viscosurgical devices, a 2-sided modified Neuhann chopper, a prebent cystotome, separate irrigation and aspiration devices, and surgical drapes.
The scissors and chopper are made of titanium and could in principle be reused, but when we finish each procedure everything is thrown away.
Weighing Pros and Cons
Now that an ASUICS pack is available, surgeons should evaluate whether this option is right for them and, above all, the best choice for their patients.
We decided in favor of single-use instruments several years ago, having evaluated the pros and cons of reusable vs single use.
The Pros
The key pros for single use include the ability to rapidly integrate updated technology without having to take a loss for outdated purchased instruments; the elimination of the risk of passing organic material from patient to patient—especially probable when having to clean a tubular instrument; the elimination of sterilization costs; and, specific to nanolaser photofragmentation, the reduced loss of endothelial cells postoperatively.
Some of the cons that must be considered include the increased cost per procedure and the increase in waste products, including packaging and instruments. We concluded that the balance was more than tipped toward a single-use solution.
We also discovered that this decision was reinforced by the rapid evolution of handpieces, which has increased the holding potential and the cataract grade that can be successfully treated without an increase in cost. This technique still has a significant margin for future developments.
Same-Day Procedures
This decision also allows to offer patients procedures for both eyes on the same day. After the first procedure is completed, the patient is moved to another operating room where a new ASUICS pack is used for the procedure on the second eye.
We have found that this option is becoming more popular with younger, active patients who must travel to my center. We also believe that the shorter recovery time that is required with a nanolaser procedure favors this option.
Although biomedical waste is an important consideration when making this decision, we believe the most pressing factors in deciding between recycling instruments or using a single-use pack should be the risk/spread of infection and the quality of the outcome.
Delaying the implementation of new technology to complete the work cycle of a reusable instrument should not be accepted under any circumstances.
Let's Check What Others Think & Say